Guidelines in Action: Flight of the Mobile Stroke Unit
A man in his 60s was flying home on an airplane when he developed acute visual disturbances followed by right facial droop, right hemiparesis, word-finding difficulty, and finally loss of consciousness. A medical emergency was activated. The flight was diverted and landed emergently. Emergency medical services (EMS) and mobile stroke unit were activated and presented on the tarmac as the flight landed. EMS and MSU teams pulled him from his airplane seat and directed him to the MSU. The National Institutes of Health Stroke Scale (NIHSS) was performed by a registered nurse aboard the MSU and a vascular neurologist present virtually. The patient was hemiplegic, grunting, and unable to follow commands, with an NIHSS score of 20. Noncontrast computed tomography (CT) head performed on the MSU demonstrated no acute hemorrhage, and thrombolysis was administered. After acute management was instituted in the MSU, he was transitioned to EMS for transport to the nearest thrombectomy-eligible hospital, given a positive prehospital screening score for a large vessel occlusion.
En route, he showed improvement in his right hemiparesis, speech, and vision deficits but continued to have a difficult time staying awake.
On arrival at the emergency room, his NIHSS score was 5 for decreased level of consciousness, partial facial weakness, limb ataxia, and dysarthria. Noncontrast CT head and CT angiogram demonstrated no hemorrhagic conversion or large vessel occlusion. He was admitted to the Neuro Intensive Care Unit. Subsequent magnetic resonance imaging brain showed an acute ischemic infarction of the bilateral medial thalami (Figure 1), consistent with infarct in the vascular territory of the artery of Percheron or tip-of-the-basilar syndrome. His discharge NIHSS score was 1 for dysarthria. At 90-day outpatient follow-up, his NIHSS score was 0, and modified Rankin Scale score was 0.
Figure 1. Axial diffusion-weighted magnetic resonance imaging showing infarction of the medial thalami.
DISCUSSION
Stroke remains a major cause of morbidity and mortality, although intravenous thrombolysis and/ or endovascular thrombectomy have been shown to improve outcomes.1 This is because <5 percent of patients receive these interventions,2 mainly due to delayed presentation from patient (onset-to-emergency call time), prehospital (onset-to-door), and intrahospital (door-to-treatment) factors.3 Less than 15% to 40% of patients with acute stroke arrive within the treatment window, and even fewer arrive within the Golden Hour. 2 The time-dependent benefit of these interventions further complicates this issue; for example, the number needed to treat for 1 excellent outcome is 4.5 when intravenous thrombolysis is given within 90 minutes versus 14 when given between 181 and 270 minutes.4
Conceptualized in 2003, the MSU was first evaluated in clinical practice in Homburg, Germany (2008), to help reduce prehospital time delay by bringing stroke treatment to the site of emergency.2 These specialized ambulances house a CT scanner, point-of-care laboratory, telemedicine connection to the hospital, advanced stroke medications, and a specialized stroke team.
Randomized trials (Walter et al2; PHANTOM-S [The Prehospital Acute Neurological Therapy and Optimization of Medical Care in Stroke Patients – Study] in Berlin) demonstrated that MSU care significantly reduces the time from symptom onset-to-intravenous thrombolysis—from 153 to 72 minutes in one study, and a 25 minutes shortening in the other—while increasing the thrombolysis rate by >50%, and the proportion of patients treated within 90 minutes of symptoms onset from 37% with usual care to 58% with MSU care, without any safety concerns.3 Based on these findings, the first MSU was launched in the United States in Houston, TX (2013)5 and since then has been successfully implemented at multiple locations across the nation. Two large prospective, nonrandomized trials with blinded outcomes assessments—B_PROUD (Berlin Prehospital or Usual Delivery of Acute Stroke Care [in Berlin, Germany]), and BEST-MSU (Benefits of Stroke Treatment Delivered by a Mobile Stroke Unit Compared With Standard Management by Emergency Medical Services [at 7 US centers, mostly Houston])—evaluated the impact of MSU on clinical outcomes and showed significant improvement in functional outcomes at 3 months in patients treated via MSU compared with Usual EMS care.1 A systematic review and meta-analysis (2022) affirmed these results and showed that, compared with EMS, MSU is associated with a 30-minute reduction in onset-to-intravenous thrombolysis time, a 65% increased odds of excellent outcomes, reduced disability at 90 days, and a higher thrombolysis rate, especially within the golden hour, all without significant safety concerns.6 Evidence is mixed on whether MSU shortens endovascular thrombectomy metrics, due largely to variations in prehospital (on-board CT angiogram) and intrahospital protocols. Studies like B_Proud and BEST-MSU found no significant association between MSU and faster dispatch-to-thrombectomy time or higher thrombectomy rates.6 However, if equipped with a CT angiogram, Czap et al7 and Zhao et al1 observed that MSU led to shorter door-to-puncture time, earlier prehospital diagnosis, direct triage to endovascular thrombectomy centers, earlier prenotification, and greater estimated disability avoidance due to earlier endovascular thrombectomy.1
Based on the recent INTERACT 4 trial (Fourth Intensive Ambulance-Delivered Blood Pressure Reduction in Hyper-Acute Stroke), MSU may be useful in intracerebral hemorrhage) management, with operational time metrics similar to acute ischemic stroke care.8 Although the B-Proud intracerebral hemorrhage subgroup saw earlier imaging and lower systolic blood pressure on arrival with MSU versus conventional care, it did not show improved outcomes. This subgroup was small (n=173) and had limitations.9 Larger studies are needed to clarify MSU’s role in intracerebral hemorrhage care.
MSUs, although successful across diverse global locations and healthcare systems, are typically located in urban areas, and cover a limited catchment area with relatively high population density. Although promising for rural areas facing treatment delays due to long drive times and lack of comprehensive stroke centers, more research is needed on their functional and economic impact in low-density or low-incidence settings.1
A prospective multicenter analysis of MSU cost-effectiveness,10 using cost data from 7 US sites, found the average annual capital investment and operation cost of an MSU was $445 812. The study concluded that MSUs are cost-effective to highly cost-effective (per World Health Organization CHOICE [Choosing Interventions That Are Cost-Effective] recommendation definitions) when calculations include patients without preexisting disability, account for stroke-related costs, use a patient’s lifetime horizon, and if the MSU treats more patients annually.
Operating an MSU program requires careful consideration of catchment area, peak coverage hours, and hardware and personnel costs—the last 2 being the biggest drivers of cost.
Personnel costs vary based on required team composition (per local regulations), use of on-board versus telemedicine specialists, and regional salaries.10 Remote telemedicine stroke neurologists offer comparable reliability and accuracy to an on-board neurologist without significant treatment delays, though technical failures remain a concern.1
Hardware costs can be reduced with less expensive drugs or diagnostic technology.10 On-board CT angiography is an option, but currently, most MSU programs do not use it due to greater requirements (patient and location-specific), and unproven cost-effectiveness.
The increased number of patients treated per year reduces cost per dispatch, but the number of potential patients is limited by the covered catchment area. This can be improved by optimizing dispatch algorithms through collaboration with EMS and local hospitals, or by employing rendezvous strategies where EMS and MSU teams meet midway.
Expanding MSU use to other neurological emergencies like traumatic brain injury, subarachnoid hemorrhage, and status epilepticus might also be helpful pending further research.10
GUIDELINE IMPLEMENTATION
In conclusion, our clinical case highlights how MSU brings acute stroke care directly to the emergency site, allows prompt management, and helps improve functional outcome without safety concerns (Figure 2). Our MSU is protocolled to dispatch in conjunction with EMS for patients with a suspected stroke. It is equipped with a CT scanner, point-of-care laboratory, advanced stroke medications, and stroke-specialized staff on-board and via telemedicine. Prehospital screening for large vessel occlusion allows appropriate triage to a thrombectomy-capable facility with prenotification of in-hospital stroke teams.
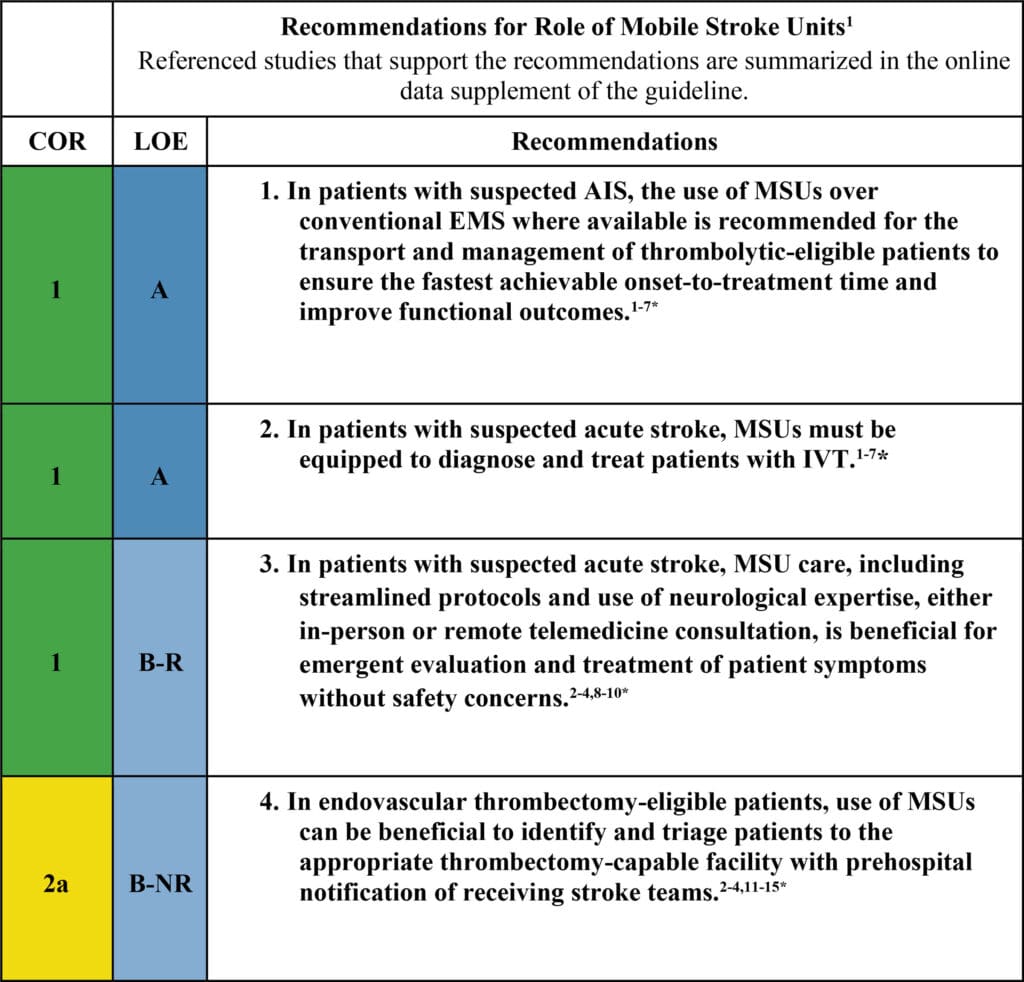
Figure 2. Recommendations for the role of mobile stroke units from the 2026 American Heart Association/American Stroke Association guideline for the early management of patients with acute ischemic stroke (AIS). B-NR indicates B-nonrandomized; B-R, B-randomized; COR, class of recommendation; EMS, emergency medical services; IVT, intravenous thrombolysis; LOE, level of evidence; and MSU, mobile stroke unit. *The references cited in the figure correspond to the references in the original guideline. Reprinted from Prabhakaran et al.1 Copyright ©2026, American Heart Association Inc.
Take-Home Points
•Mobile stroke units are specialized ambulances, usually equipped with a computed tomography scanner, a point-of-care laboratory, advanced stroke care medications, and a dedicated stroke team.
•Prehospital acute ischemic stroke management via mobile stroke units results in a reduction in time to intravenous thrombolysis, an increase in thrombolysis rate, and an improvement in 90-day functional outcomes without significant adverse effects.
•When equipped with a computed tomography angiogram, the mobile stroke unit helps with accurate triage of patients with a large vessel occlusion and helps decrease the door-to-puncture time.
•Further research will help identify the ideal setting for mobile stroke units, their impact on patients with large vessel occlusion and intracerebral hemorrhage, their long-term health economic outcomes, and their potential expansion to other neurological emergencies.
ARTICLE INFORMATION
Acknowledgements
The authors acknowledge the teams that took expedited care of the patient. All work was performed at the Department of Neurology, Barrow Neurological Institute, Phoenix, AZ.